Any time there is something in the brain that shouldn’t be there (i.e., a tumor), pressure in the brain rises. However, with pseudotumor cerebri, the pressure exists in the absence of a tumor or other mass lesion. “Imaging oftentimes does not show a tumor or any visible problem, but there are signs that there is pressure in the brain,” says endovascular neurosurgeon Kenneth Liu, MD.
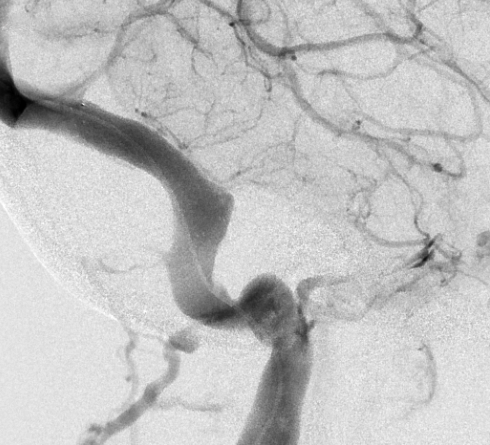
While all causes of pseudotumor cerebri have yet to be been identified, it has been revealed that some cases are the result of intracranial venous outflow stenosis. This narrowing of veins prevents adequate blood drainage from the brain. “If the blood can’t get out, it backs up, and the pressure builds,” says Liu. “Over time, this can lead to vision loss or other neurologic problems.”
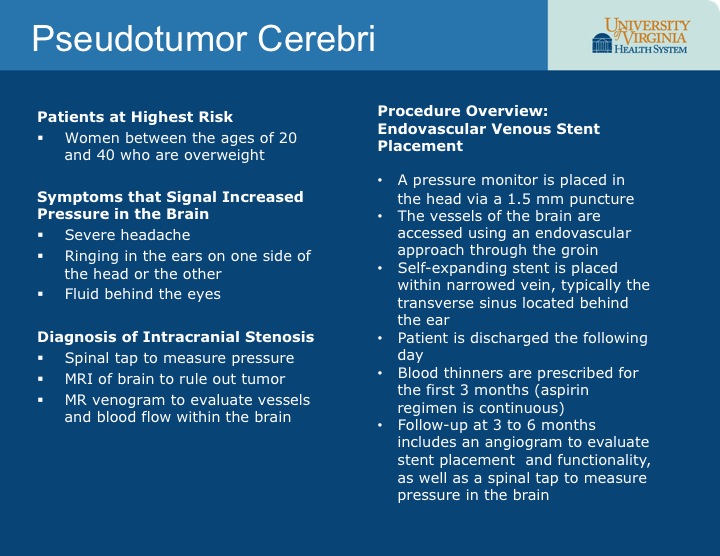
Treatments for this condition have been limited thus far to relieving the symptoms, which mimic those of a brain tumor and include severe headaches, nausea, vomiting and pulse-synchronous tinnitus. “Treatments offered thus far have not been ideal,” says Liu. “We can remove spinal fluid to compensate for the increase in pressure and patients experience some relief, but it is only temporary. Treating headaches medically may work for a while, but you’re still not treating the source of the problem.”
{kind=link}
Using Stents to Reduce Pressure
For patients with pseudotumor cerebri resulting from intracranial venous stenosis, Liu and his colleagues at UVA are now utilizing endovascular venous stent placement with positive, longer-term results. According to Liu, this technique has slowly been gaining acceptance in the past decade, and UVA is working to prove that stent placement actually reduces a patient’s intracranial pressures.
“At UVA, we are proving that stent placement reduces pressure by utilizing a pressure monitor,” he says. “Before the procedure, we implant a monitor into the brain that transduces intracranial pressures and provides a baseline measurement. We then perform the procedure with the monitor in place. Even with patients on antiplatelet therapy, we have found that the added risk of placing an invasive monitor is almost negligible and is far outweighed by the benefit of being able to measure intracranial pressures in real time before, during and after stent placement.
“So far, we are seeing immediate results,” adds Liu. “In the past year, among those patients who have undergone concomitant pressure monitoring during stent placement, all have had their intracranial pressures return to normal within one to two hours after their procedure. This is the first time we have definitive and consistent proof that improving venous outflow with stent placement normalizes a patient’s intracranial pressures.”
Promising Early Results for Symptom Relief
For approximately 50 percent of patients, the procedure is also relieving what is the most bothersome symptom for many: severe headaches. “This procedure is not designed to fix headaches — it is meant to relieve pressure in the brain and prevent blindness, which it is proving to do successfully,” says Liu. “If the headaches go away, that is a positive side effect.”
After this procedure, patients are monitored for the development of scar tissue at the stent site; their tolerance of blood thinners, which are required temporarily after surgery; and any other signs of complications. “Because this is a relatively new procedure, we are monitoring these patients very closely; we don’t have good data on how stents behave in cerebral veins,” says Liu. “There actually isn’t a large stent designed for use in the brain so we use ones designed for the carotid or iliac artery. So far, we have had no problems. Patients I treated 10 years ago have not needed a repeat procedure. However, whether the stent will be well tolerated over the long term is still unknown.”
To determine if your patient may have pseudotumor cerebri and is a candidate for endovascular stent placement, review the graphic below then contact Liu at 434.924.2735 or kenneth.c.liu@virginia.edu to arrange a consultation.
Read about one patient’s experience with pseudotumor cerebri.
{kind=link}